

By: Edgar Michael “Gar” T. Eufemio, M.D.

An athlete does not need to have a medical background to know that an Anterior Cruciate Ligament or an ACL tear is a serious problem. Every now and then, we hear about an elite player who suffers a knee injury – from basketball, volleyball or football – and we all wonder if he or she will ever get back to previous levels. For those of you who have witnessed it live and saw your teammate or opponent crumble to the ground in agony, you realize this is a bad situation…
What are some of the things we understand about the ACL? We are aware it probably needs surgery and it will be some time before the patient goes back to sports.
The questions I am hoping to answer with this piece are:
1) Why did it happen?
2) What has to be done?
3) How long before patients can return to previous level?
4) How do we prevent it from happening again?
The ACL is easily the most studied ligament in Sports Medicine. Its primary function is to prevent the leg from translating too far forward relative to the thigh. Billions have been spent on research, and treatment options continue to evolve to this day. Everything from the type of graft (the tissue or material used to replace the ruptured ACL)… to the placement of the tunnels (position of the graft in the knee)… to the implants used to hold the graft in place… to the way the knee is rehabilitated, will vary among Surgeons.
An ACL-deficient knee is unable to perform pivoting movements properly. Patients complain that their knees “give way” or “bumibigay” on certain activities. There may be locking episodes, frequent swelling and pain. Left alone, without a change in lifestyle, may result in early onset of osteoarthritis.
Ask basketball players who continue to play with a torn ACL and they will tell you that their outside shooting has improved and they play better defense now with their hands because they cannot do lateral actions confidently. Obviously, they become “dirtier” competitors too…
Volleyballers are hesitant to go for spikes or blocks and will not dive on the court…
Soccer enthusiasts cannot defend and attack confidently and stop attempting the long ball…


The same goes with all sports where rapid shifting is critical for success; performance suffers.
So why and how did it happen? This can be partly explained anatomically. Given the same exposure to sports, females are more prone to ACL tears. Due to larger hips (for childbearing purposes), women tend to be knock-kneed, and this angle predisposes them to harm. A discrepancy in quadriceps to hamstring strength is another risk factor (it is important to have strong hamstring muscles). Poor balance and lack of coordination and training have also been implicated, but we constantly read of top competitors getting an ACL tear. Surely, they were not lacking in preparation and are in great physical condition. Overtraining, repetitive stresses and a poor understanding of recovery must be considered.
Diet? Hormonal imbalance? Maybe.
For me, it is still fate or bad luck. It just happens – wrong movement, bad landing and the perfect angle… The ACL snaps.
So, what’s next? All studies support the need for surgery. Newer papers show good results repairing the ligament or simply immobilizing the knee at a certain angle. These are for selected cases and needed to be followed up further. Due to its precarious blood supply, most ACL tears do not heal, so they must be replaced or reconstructed.
There are four requirements before surgery can be performed:
1) Knee extension must be normal
2) Knee flexion should be equal or within 10 degrees of the uninjured side
3) Minimal swelling
4) Normal walking without assistive devices
These must be achieved to avoid excessive scar tissue formation, which prevents normal range of motion and delays rehabilitation.



Once you have accepted that you will need that trip to the Operating Room, more inquiries will crop up…
“Where will the graft come from?”
“What type of implant will be used?”
“What technique?”
“What type of Anesthesia?”
“Will I need to be admitted?”
“How long will the incision be?”
“Where did my Surgeon train?”
“How many cases has he or she done?”
“How much will I have to prepare?”
“How painful will it be?”
“How will I take a shower after?”
“Can I take alcohol post-op?”
“When can I walk, go back to work or school, drive and exercise?”
“What about sex?”
And the most important question, “When can I go back to sports?”
Your surgeon should be able to answer all of these. The choice of graft, implant and technique is quite technical. Listen carefully…
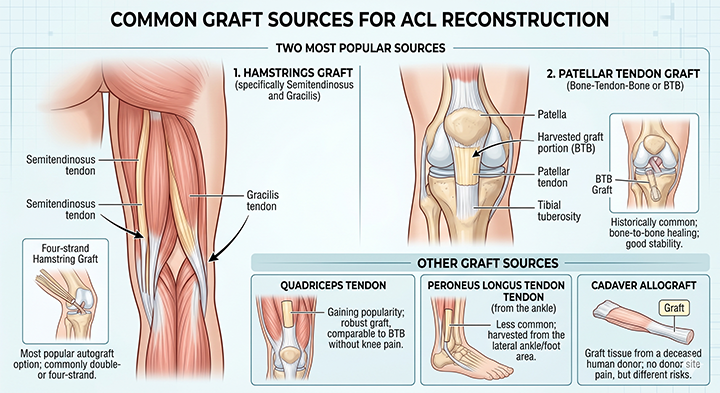
The two most popular sources for the new ACL are the hamstrings (specifically the semitendinosus and gracilis tendons) and the patellar tendon. Other sources include the quadriceps tendon, the peroneus longs tendon (from the ankle) and a cadaver allograft.
The commonly used implants are suspensory devices and screws.
My preference is the semitendinosus, folded twice to produce four strands (I spare the gracilis). I use a titanium or a resorbable plastic screw on the femur (the thigh end) and a button on the tibia (the leg). No reason. I am used to it, I am happy with my results and I can do it in the shortest possible time. I complement my reconstruction with an internal brace. It is like adding a seat belt for added protection.
During my stint as the Head of the UP-PGH Sports Clinic (2000-2010), I developed an implant-less procedure to help our indigent countrymen. It is also my technique-of-choice for patients who have a re-tear following a reconstruction using the hamstrings.
As Surgeons, we can only hope to approximate the strength of the native ligament. If the “original”, that God gave you, tore, then definitely a man-made ACL cannot be better.
Depending on the post-operative program that you follow, patients can go back to competitive sports from eight to twelve months.
Highlights of my protocol:
• Full weight bearing as early as two hours after surgery
• Knee bent to 90 degrees the day after
• Biking at two weeks
• Weights at four weeks
• Running at three months
• Trampoline at four months
• Sports-specific drills at five months
• Scrimmages at six months
• Back to sports at eight months
Never forget, an ounce of prevention is better than a pound of cure. Look back at all the possible causes of an ACL tear. Some are modifiable. Strengthen the hamstrings, work on flexibility, improve core strength, and develop better balance and landing skills.
An ACL tear used to be the end of a sporting career. Nowadays, with the proper mix of a seasoned Surgeon, a skilled Rehab Doctor, modern-day Physical Therapists and Conditioning Coaches, supportive family members, encouraging friends and a determined patient, a full recovery is not just a possibility; it is the norm.









Leave a Reply